State Form
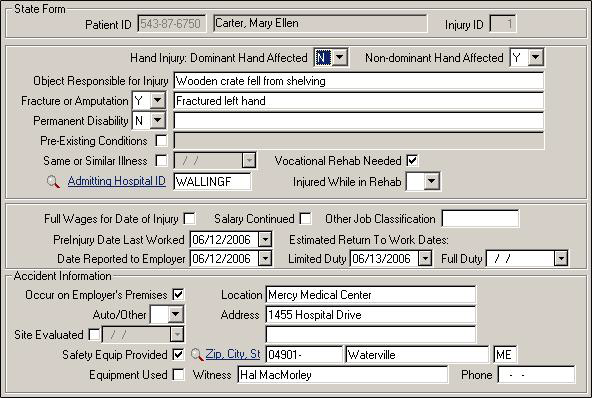
The State Form screen contains information that is required for injury and claim reports in various states. Use as few or as many of the fields as you need for reporting purposes.
| Label | Description |
|---|---|
|
Injury ID |
Check to ensure you are working on the appropriate ID for patients who may have multiple injury IDs. |
|
Dominant/Non-dominant |
For hand injuries, indicate which hand was affected (for a right-handed person, the right hand is dominant, the left is non-dominant). Use drop-down lists to indicate Y for Yes, N for No, or leave blank. |
|
Object Responsible |
Describe the object that caused the accident, if any. |
|
Fracture/Amputation |
If the injury is a fracture or amputation, select Y and describe in the adjacent field. |
|
Permanent Disability |
If the disability is believed to be permanent, select Y and give further details in the adjacent field. |
|
Pre-Existing Conditions |
Mark this box if pre-existing conditions were a factor in this incident, and describe in the adjacent field. |
|
Same or Similar Illness |
Check the box if it is a recurrence of a former incident and enter the original injury date in the adjacent field. |
|
Admitting Hospital ID |
Link to to select the ID of the facility, if the patient was admitted to a hospital. |
|
Vocational Rehab Needed |
If vocational rehabilitation is needed, check the box. |
|
Injured While in Rehab |
From the drop-down list, choose Y, N, or leave blank to indicate if the patient was injured during a rehabilitation session. |
|
Full Wages |
Check the box if the patient was paid in full for the day on which s/he was injured. |
|
Salary Continued |
Check the box if the company continued to pay the patient's salary after the injury. |
|
Other Job Classification |
If your state has additional job coding, indicate the appropriate code here. |
|
PreInj. Date Last Worked |
Actual last date injured worker performed normal job duties prior to his/her injury. Over the life of the claim, you may need to enter multiple last days worked if the injured worker has multiple periods of disability. |
|
Date Reported to Emp. |
Date the injury was first reported to the employer. |
|
Estimated RTW Dates |
Dates the patient is likely to return to work with limited duty or full duty. |
|
Occur on Emp. Premises |
Check if the injury occurred on the employer's premises; the location fields are then automatically entered based on the Company ID from the injury screen. |
|
Location |
Place where accident occurred. If you check the 'Occur on Employer's Premises' field, the location is automatically filled. |
|
Auto/Other |
Accident type: A for auto accident, O for other type
of accident, or leave blank. If you use SYSTOC_EDI for billing,
you must select the appropriate accident type if the claim is an
accident. Note: Changing the field and saving
this screen updates the same field on the Injury screen.
|
|
Site Evaluated |
If the injury site was evaluated, check the field and indicate the date of evaluation. |
|
Safety Equip Provided |
Check the field if the employer provided safety equipment to this employee. |
|
Equipment Used |
Check the field if the patient was using safety equipment at the time of the accident. |
|
Witness |
Name of the witness to the incident, if any. |
|
Phone |
Telephone number of the witness, if any. |