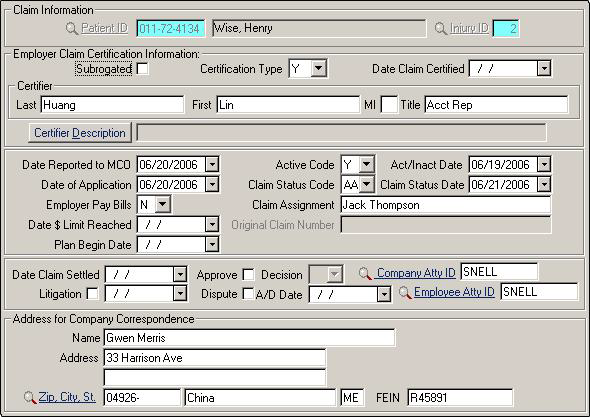
Claim Information
This screen contains much of the data you may need for complex claims, especially if litigation is involved.
| Label | Description |
|---|---|
|
Injury ID |
Check to ensure you are working on the appropriate injury for patients who may have more than one injury record. |
|
Subrogated |
Check this box if the employer or insurer is entitled to reimbursement for money paid in medical and lost-time benefits for the injured worker, based on receiving funds later from another source. |
|
Certification Type |
Does the employer accept the certification of the claim as a workers' compensation case?
|
|
Date Claim Certified |
Date the claim was certified by the employer as a workers' comp case. |
|
Certifier |
Full name and title of company representative. |
|
Certifier Description |
Memo where you can record the employer's rationale for allowing the claim for certain listed conditions or enter other remarks pertinent to the claim. |
|
Date Reported to MCO |
Date the clinic reported the injury to the appropriate agency. Providers are sometimes required to report the employee's injury to an MCO or a state agency within a specified time after the initial treatment or visit. |
|
Active Code |
Does an active claim exist? Enter Y, N, or leave blank. Claims with activity within a period defined by the insurer are considered active claims. Claims with no activity within a period of time defined by the insurer are considered inactive. |
|
Act/Inact Date |
Date the Active/Inactive status took effect. |
|
Date of Application |
Date the claim was filed with the insurer. |
|
Claim Status Code |
Status of the claim after the insurer has completed an initial investigation of the claim. Choose from 14 possible codes from the drop-down list (a description of each appears in the status bar in the upper right portion of your screen). |
|
Claim Status Date |
Date associated with the status code of the claim. |
|
Employer Pay Bills |
Enter Y if the employer pays medical bills associated with this injury, N if the employer does not pay the bills. |
|
Claim Assignment |
Upon receipt of the First Notice of Injury the claim is assigned to insurer representatives who determine compensation issues. Enter the name of the person assigned. |
|
Date $ Limit Reached |
If the employer is paying the medical bills for the injury and has reached the payment limit, enter the date here. |
|
Original Claim Number |
Original claim number issued when you first record an injury in the Injuries table. This field is not editable. |
|
Plan Begin Date |
Date the medical management of the claim began. |
|
Date Claim Settled |
Date of agreement among the insurer, employer, and injured worker to pay a sum of money to resolve all past, present, or future medical liabilities of the claim. |
|
Approve |
Check the box if the claim is approved as a workers' comp accident by the company, insurer, etc. |
|
Decision |
If the Dispute field has been checked, the result of the dispute should be entered here. From the drop-down list, choose A if the claim is accepted, D if the claim is denied, or leave blank if there is no decision yet. |
|
Company Atty ID |
Link to to select the legal representative for the company for this injury. |
|
Litigation |
Check if any legal action has been filed in this case and enter the date in the adjacent field. |
|
Dispute |
Check if the denial of the claim has been disputed. |
|
A/D Date |
Date the claim was approved or denied. |
|
Employee Atty ID |
Link to to select the legal representative for the patient for this injury. |
|
Company Correspondence |
For the company responsible for this claim, enter the contact person, address, and FEIN. |